Watchers of ‘House MD’, the popular American medical serial would, unlike the general public, be very familiar with the term ‘Guillain–Barré syndrome’. GBS is a rare neurological autoimmune disorder in which a person’s immune system mistakenly attacks part of their own peripheral nervous system—the network of nerves which carry signals from the brain and spinal cord to the rest of the body. This can result in muscle weakness, loss of sensation in the legs and/or arms, and problems swallowing or breathing. Symptoms typically last a few weeks, with most individuals recovering without long-term, severe neurological complications.
The cause of GBS is not fully understood, but most cases follow after a viral or bacterial infection. Infection with the bacteria Campylobacter jejuni, which causes gastroenteritis (including symptoms of nausea, vomiting and diarrhoea), is one of the most common risk factors for GBS. People could also develop GBS after having the flu or other viral infections including cytomegalovirus, Epstein-Barr virus, and the Zika virus.
GBS is rare, affecting about 1 in 78,000 people across the world each year. But in the last few weeks, over 150 cases have been detected in India, especially in and around Pune and Maharashtra. Of concern is that a case has been detected as far away as Assam. A few deaths have also resulted.
Authorities are fully alert and taking action—both to ensure detection and treatment, but also importantly, prevention. Pune Municipal Corporation is promoting public health interventions – food and hand hygiene, and safe water — for disease management.
But getting back to ‘House MD’, so influential was the serial, that there is actually an academic paper titled ‘The usefulness of TV medical dramas for teaching clinical pharmacology: A content analysis of House M.D’, in a respected medical journal ‘Educacion Medica’!
Of course such serials often have patients misdiagnosing themselves with all kinds of exotic diseases, and generally being a pain in the neck for doctors, and a waste of resources. But in the case of one patient, Alexandria Ostrem, it was a tale stranger than fiction. Way back in 2008, when Alexandria was a teenager and an avid watcher of House. she suddenly developed trouble walking. Remembering the symptoms of GBS from all her TV-viewing, she rushed to the emergency room and insisted that the doctors test her for the syndrome. However, the results came back negative.
Her symptoms continued to worsen, and she was tested several times for GBS. But nothing positive showed up. There came a stage when she was paralyzed nearly everywhere except for some use of her arms. At this point, doctors told her they agreed with her self-diagnosis, and started treating her for GBS. She responded and got well!
In the serial House MD, the doctor and his team are super-specialists in rare diseases, and when diagnosing, they tend to think in terms of unusual and exotic diseases. Such diagnosticians are called ‘zebra hunters’, a term for someone who foolishly chooses to seek out the rarest of diseases. In the normal course of things, doctors are trained to do the opposite– summed up by the adage, “If you hear hoof-beats, think horses, not zebras.”
We are fortunate that the doctors in our health system listened to the hoof-beats carefully, and identified the zebras! Thank you all healthcare givers for all that you do for us.
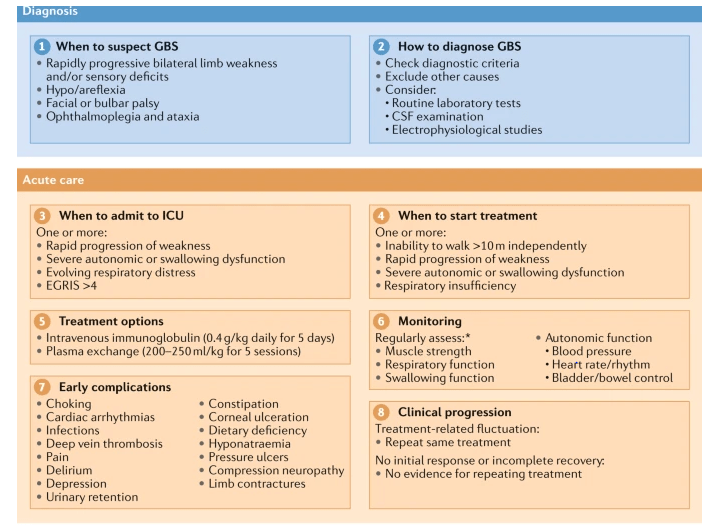
Leonhard, S.E., Mandarakas, M.R., Gondim, F.A.A. et al. Diagnosis and management of Guillain–Barré syndrome in ten steps. Nat Rev Neurol 15, 671–683 (2019). https://doi.org/10.1038/s41582-019-0250-9
And here is praying that all those who have contracted GBS may recover quickly.
–Meena
The author is a laymen. All information is quoted from sources perceived to be authentic, and should not be a basis for action.
http://www.my.clevelandclinic.org/health/diseases/
http://www.who.int/news-room/fact-sheets/detail/guillain-barr%C3%A9-syndrome